Fauci’s NIH Research Proves 5G Spiked Sars Cov 2 Breakout in Wuhan and Globally-Proving 5G is Deadly.
Sun 10:08 pm +00:00, 26 Dec 2021
Fauci’s NIH Research Proves 5G Spiked Sars Cov 2 Breakout in Wuhan and Globally-Proving 5G is Deadly.
Confirming our Warnings. Published online Sept. 29, 2021
Fifth Generation [5G] Wireless Communications Radiation [WCR]) and (SARS-CoV-2) Virus and its Effects on Human Health
Journal of Clinical and Translational Research Evidence for a Connection between Coronavirus Disease-19 and 5G Exposure
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8580522/
Evidence for a connection between coronavirus disease-19 and exposure to radiofrequency radiation from wireless communications including 5G (WCR) Wireless Communication Radiation
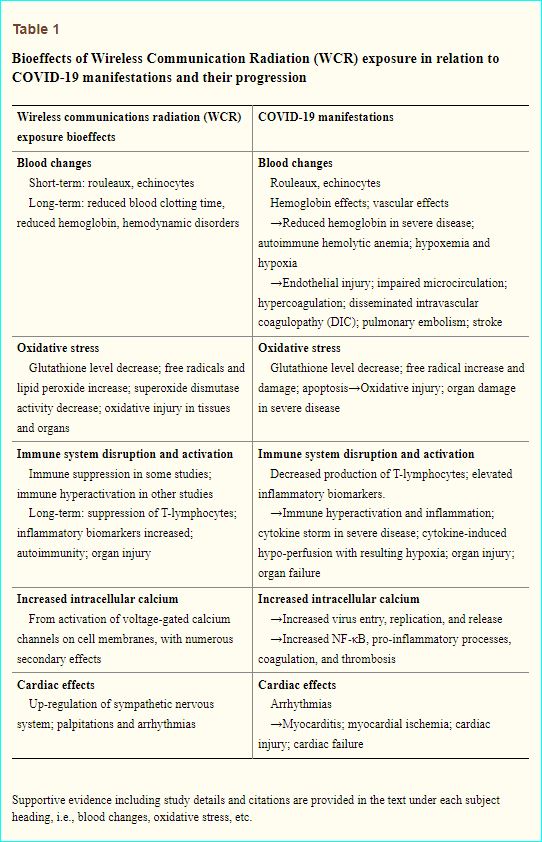
Both COVID-19 and WCR Wireless Communication Radiation Exposure Can Affect the Heart and Cardiovascular System, Directly and/or Indirectly
5. Conclusion
There is a substantial overlap in pathobiology between COVID-19 and WCR exposure. The evidence presented here indicates that mechanisms involved in the clinical progression of COVID-19 could also be generated, according to experimental data, by WCR exposure.
Therefore, we propose a link between adverse bioeffects of WCR exposure from wireless devices and COVID-19.
Specifically, evidence presented here supports a premise that WCR and, in particular, 5G, which involves densification of 4G, may have exacerbated the COVID-19 pandemic by weakening host immunity and increasing SARS-CoV-2 virulence by (1) causing morphologic changes in erythrocytes including echinocyte and rouleaux formation that may be contributing to hypercoagulation; (2) impairing microcirculation and reducing erythrocyte and hemoglobin levels exacerbating hypoxia; (3) amplifying immune dysfunction, including immunosuppression, autoimmunity, and hyperinflammation; (4) increasing cellular oxidative stress and the production of free radicals exacerbating vascular injury and organ damage; (5) increasing intracellular Ca2+ essential for viral entry, replication, and release, in addition to promoting pro-inflammatory pathways; and (6) worsening heart arrhythmias and cardiac disorders.
WCR exposure is a widespread, yet often neglected, environmental stressor that can produce a wide range of adverse bioeffects. For decades, independent research scientists worldwide have emphasized the health risks and cumulative damage caused by WCR [42,45]. The evidence presented here is consistent with a large body of established research.
Healthcare workers and policymakers should consider WCR a potentially toxic environmental stressor.
Methods for reducing WCR exposure should be provided to all patients and the general population.
************************************
Scientific Study Concludes That 5G Exacerbated COVID / Reese Report
*************************
KEY POINTS ARE LISTED BELOW, BUT I RECOMMEND READING THE ENTIRE DOCUMENT AND SHARING THIS EXPLOSIVE REPORT EVERYWHERE POSSIBLE
COVID-19 began in Wuhan, China in December 2019, shortly after city-wide 5G had “gone live,” that is, become an operational system, on October 31, 2019. COVID-19 outbreaks soon followed in other areas where 5G had also been at least partially implemented, including South Korea, Northern Italy, New York City, Seattle, and Southern California.
In May 2020, Mordachev [4] reported a statistically significant correlation between the intensity of radiofrequency radiation and the mortality from SARS-CoV-2 in 31 countries throughout the world.
During the first pandemic wave in the United States, COVID-19 attributed cases and deaths were statistically higher in states and major cities with 5G infrastructure as compared with states and cities that did not yet have this technology [5].
There is a large body of peer reviewed literature, since before World War II, on the biological effects of WCR that impact many aspects of our health. In examining this literature, we found intersections between the pathophysiology of SARS-CoV-2 and detrimental bioeffects of WCR exposure. Here, we present the evidence suggesting that WCR has been a possible contributing factor exacerbating COVID-19.
Sars Cov 2 / Covid-19 and 5G Radiation Share Most of the Same Symptoms
1.2. Overview on COVID-19
The clinical presentation of COVID-19 has proven to be highly variable, with a wide range of symptoms and variability from case to case.
According to the CDC, early disease symptoms may include sore throat, headache, fever, cough, chills, among others. More severe symptoms including shortness of breath, high fever, and severe fatigue may occur in a later stage. The neurological sequela of taste and smell loss has also been described.
Ing et al. [6] determined 80% of those affected have mild symptoms or none, but older populations and those with comorbidities, such as hypertension, diabetes, and obesity, have a greater risk for severe disease [7]. Acute respiratory distress syndrome (ARDS) can rapidly occur [8] and cause severe shortness of breath as endothelial cells lining blood vessels and epithelial cells lining airways lose their integrity, and protein rich fluid leaks into adjacent air sacs. COVID-19 can cause insufficient oxygen levels (hypoxia) that have been seen in up to 80% of intensive care unit (ICU) patients [9] exhibiting respiratory distress. Decreased oxygenation and elevated carbon dioxide levels in patients’ blood have been observed, although the etiology for these findings remains unclear.
Massive oxidative damage to the lungs has been observed in areas of airspace opacification documented on chest radiographs and computed tomography (CT) scans in patients with SARS-CoV-2 pneumonia [10]. This cellular stress may indicate a biochemical rather than a viral etiology [11].
1.3. Overview on bioeffects of WCR Wireless Communications Radiation exposure
In 2009, Johansson conducted a literature review, which included the 2007 Bioinitiative Report. He concluded that electromagnetic fields (EMF) exposure, including WCR, can disturb the immune system and cause allergic and inflammatory responses at exposure levels significantly less than current national and international safety limits and raise the risk for systemic disease
Organisms are electrochemical beings. Low-level WCR from devices, including mobile telephony base antennas, wireless network protocols utilized for the local networking of devices and internet access, trademarked as Wi-Fi (officially IEEE 802.11b Direct Sequence protocol; IEEE, Institute of Electrical and Electronic Engineers) by the Wi-Fi alliance, and mobile phones, among others, may disrupt regulation of numerous physiological functions.
Non-thermal bioeffects (below the power density that causes tissue heating) from very low-level WCR exposure have been reported in numerous peer-reviewed scientific publications at power densities below the International Commission on Non-Ionizing Radiation Protection (ICNIRP) exposure guidelines [14]. Low-level WCR has been found to impact the organism at all levels of organization, from the molecular to the cellular, physiological, behavioral, and psychological levels.
Moreover, WCR has been shown to cause systemic detrimental health effects including increased cancer risk [15], endocrine changes [16], increased free radical production [17], deoxyribonucleic acid (DNA) damage [18], changes to the reproductive system [19], learning and memory defects [20], and neurological disorders [21].
Having evolved within Earth’s extremely low-level natural radiofrequency background, organisms lack the ability to adapt to heightened levels of unnatural radiation of wireless communications technology with digital modulation that includes short intense pulses (bursts).
In considering the epidemiological triad (agent-host-environment) applicable to all disease, we investigated a possible environmental factor in the COVID-19 pandemic: ambient radiofrequency radiation from wireless communication systems including microwaves and millimeter waves.
SARS-CoV-2, the virus that caused the COVID-19 pandemic, surfaced in Wuhan, China shortly after the implementation of city-wide (fifth generation [5G] of wireless communications radiation [WCR]), and rapidly spread globally, initially demonstrating a statistical correlation to international communities with recently established 5G networks
Demonstrating a statistical correlation to international communities with recently established 5G networks
We explore the scientific evidence suggesting a possible relationship between COVID-19 and radiofrequency radiation related to wireless communications technology including fifth generation (5G) of wireless communications technology, henceforth referred to as WCR. WCR has already been recognized as a form of environmental pollution and physiological stressor [2]. Assessing the potentially detrimental health effects of WCR may be crucial to develop an effective, rational public health policy that may help expedite eradication of the COVID-19 pandemic. In addition, because we are on the verge of worldwide 5G deployment, it is critical to consider the possible damaging health effects of WCR before the public is potentially harmed.
5G is a protocol that will use high frequency bands and extensive bandwidths of the electromagnetic spectrum in the vast radiofrequency range from 600 MHz to nearly 100 GHz, which includes millimeter waves (>20 GHz), in addition to the currently used third generation (3G) and fourth generation (4G) long-term evolution (LTE) microwave bands.
5G frequency spectrum allocations differ from country to country.
Focused pulsed beams of radiation will emit from new base stations and phased array antennas placed close to buildings whenever persons access the 5G network.
Because these high frequencies are strongly absorbed by the atmosphere and especially during rain, a transmitter’s range is limited to 300 meters.
Therefore, 5G requires base stations and antennas to be much more closely spaced than previous generations. Plus, satellites in space will emit 5G bands globally to create a wireless worldwide web.
The new system therefore requires significant densification of 4G infrastructure as well as new 5G antennas that may dramatically increase the population’s WCR exposure both inside structures and outdoors.
Approximately 100,000 emitting satellites are planned to be launched into orbit. This infrastructure will significantly alter the world’s electromagnetic environment to unprecedented levels and may cause unknown consequences to the entire biosphere, including humans.
The new infrastructure will service the new 5G devices, including 5G mobile phones, routers, computers, tablets, self-driving vehicles, machine-to-machine communications, and the Internet of Things.
The global industry standard for 5G is set by the 3G Partnership Project (3GPP), which is an umbrella term for several organizations developing standard protocols for mobile telecommunications.
The 5G standard specifies all key aspects of the technology, including frequency spectrum allocation, beam-forming, beam steering, multiplexing multiple in, multiple out schemes, as well as modulation schemes, among others.
5G will utilize from 64 to 256 antennas at short distances to serve virtually simultaneously a large number of devices within a cell. The latest finalized 5G standard, Release 16, is codified in the 3GPP published Technical Report TR 21.916 and may be downloaded from the 3GPP server at https://www.3gpp.org/specifications.
Engineers claim that 5G will offer performance up to 10 times that of current 4G networks [3].
(Continued below)
*************************************

Covid-19 no longer a threat in Ireland after 5G towers burn
https://thedailyirish.weebly.com/blog/covid-19-no-longer-a-threat-in-ireland-after-5g-towers-burn
NIH REPORT TRIES TO DICREDIT THE CONNECTION BETWEEN 5G AND COVID-19
(That’s Right. They can Report the Truth on Their Website, But they Have To Discredit the Public Reports AS CONSPIRACY THEORY)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7205032/
COVID-19 and the 5G Conspiracy Theory: Social Network Analysis of Twitter Data
Abstract / Background
Since the beginning of December 2019, the coronavirus disease (COVID-19) has spread rapidly around the world, which has led to increased discussions across online platforms. These conversations have also included various conspiracies shared by social media users. Amongst them, a popular theory has linked 5G to the spread of COVID-19, leading to misinformation and the burning of 5G towers in the United Kingdom. The understanding of the drivers of fake news and quick policies oriented to isolate and rebate misinformation are keys to combating it.
(1).jpg)
WHY DOES 5G TRANSMITTER HAVE A COVID-19 DESIGNATION?
*********************************
(Continued from above)
3.3. Immune system disruption and activation
When SARS-CoV-2 first infects the human body, it attacks cells lining the nose, throat, and upper airway harboring ACE2 receptors. Once the virus gains access to a host cell through one of its spike proteins, which are the multiple protuberances projecting from the viral envelope that bind to ACE2 receptors, it converts the cell into a virus self-replicating entity.
In response to COVID-19 infection, both an immediate systemic innate immune response as well as a delayed adaptive response has been shown to occur [93]. The virus can also cause a dysregulation of the immune response, particularly in the decreased production of T-lymphocytes. [94]. Severe cases tend to have lower lymphocyte counts, higher leukocyte counts and neutrophil-lymphocyte ratios, as well as lower percentages of monocytes, eosinophils, and basophils [94]. Severe cases of COVID-19 show the greatest impairment in T-lymphocytes.
In comparison, low-level WCR studies on laboratory animals also show impaired immune function [95]. Findings include physical alterations in immune cells, a degradation of immunological responses, inflammation, and tissue damage. Baranski [96] exposed guinea pigs and rabbits to continuous or pulse-modulated 3000 MHz microwaves at an average power density of 3.5 mW/cm2 for 3 h/day over 3 months and found nonthermal changes in lymphocyte counts, abnormalities in nuclear structure, and mitosis in the erythroblastic cell series in the bone marrow and in lymphoid cells in lymph nodes and spleen. Other investigators have shown diminished T-lymphocytes or suppressed immune function in animals exposed to WCR. Rabbits exposed to 2.1 GHz at 5mW/cm2 for 3 h/day, 6 days/week, for 3 months, showed suppression of T-lymphocytes [97]. Rats exposed to 2.45 GHz and 9.7 GHz for 2 h/day, 7 days/week, for 21 months showed a significant decrease in the levels of lymphocytes and an increase in mortality at 25 months in the irradiated group [98]. Lymphocytes harvested from rabbits irradiated with 2.45 GHz for 23 h/day for 6 months show a significant suppression in immune response to a mitogen [99].
In 2009, Johansson conducted a literature review, which included the 2007 Bioinitiative Report. He concluded that electromagnetic fields (EMF) exposure, including WCR, can disturb the immune system and cause allergic and inflammatory responses at exposure levels significantly less than current national and international safety limits and raise the risk for systemic disease
COVID-19 patients commonly show increased levels of cardiac troponin, indicating damage to the heart muscle [122]. Cardiac damage has been associated with arrhythmias and increased mortality. Cardiac injury is thought to be more often secondary to pulmonary emboli and viral sepsis, but direct infection of the heart, that is, myocarditis, can occur through direct viral binding to ACE2 receptors on cardiac pericytes, affecting local, and regional cardiac blood flow [60].
Immune system activation along with alterations in the immune system may result in atherosclerotic plaque instability and vulnerability, that is, presenting an increased risk for thrombus formation, and contributing to development of acute coronary events and cardiovascular disease in COVID-19.
Regarding WCR exposure bioeffects, in 1969 Christopher Dodge of the Biosciences Division, U.S. Naval Observatory in Washington DC, reviewed 54 papers and reported that radiofrequency radiation can adversely affect all major systems of the body, including impeding blood circulation; altering blood pressure and heart rate; affecting electrocardiograph readings; and causing chest pain and heart palpitations [123]. In the 1970s Glaser reviewed more than 2000 publications on radiofrequency radiation exposure bioeffects and concluded that microwave radiation can alter the electrocardiogram, cause chest pain, hypercoagulation, thrombosis, and hypertension in addition to myocardial infarction [27,28]. Seizures, convulsions, and alteration of the autonomic nervous system response (increased sympathetic stress response) have also been observed.
Since then, many other researchers have concluded that WCR exposure can affect the cardiovascular system. Although the nature of the primary response to millimeter waves and consequent events are poorly understood, a possible role for receptor structures and neural pathways in the development of continuous millimeter wave-induced arrhythmia has been proposed [47].
In 1997, a review reported that some investigators discovered cardiovascular changes including arrhythmias in humans from long-term low-level exposure to WCR including microwaves [124]. However, the literature also shows some unconfirmed findings as well as some contradictory findings [125].
Havas et al. [126] reported that human subjects in a controlled, double-blinded study were hyper-reactive when exposed to 2.45 GHz, digitally pulsed (100 Hz) microwave radiation, developing either an arrhythmia or tachycardia and upregulation of the sympathetic nervous system, which is associated with the stress response.
Saili et al. [127] found that exposure to Wi-Fi (2.45 GHz pulsed at 10 Hz) affects heart rhythm, blood pressure, and the efficacy of catecholamines on the cardiovascular system, indicating that WCR can act directly and/or indirectly on the cardiovascular system.
Most recently, Bandara and Weller [91] present evidence that people who live near radar installations (millimeter waves: 5G frequencies) have a greater risk of developing cancer and experiencing heart attacks.
Similarly, those occupationally exposed have a greater risk of coronary heart disease. Microwave radiation affects the heart, and some people are more vulnerable if they have an underlying heart abnormality [128]. More recent research suggests that millimeter waves may act directly on the pacemaker cells of the sinoatrial node of the heart to change the beat frequency, which may underlie arrhythmias and other cardiac issues [47].
In short, both COVID-19 and WCR exposure can affect the heart and cardiovascular system, directly and/or indirectly.
https://beforeitsnews.com/alternative/2021/12/faucis-nih-research-proves-5g-spiked-sars-cov-2-breakout-in-wuhan-and-globally-proving-5g-is-deadly-confirming-our-warnings-published-online-sept-29-2021-3764220.html