BBC Covid ‘Reality Check’ Needs a Fact Check of Its Own
Wed 10:58 am +01:00, 24 Mar 2021
In its latest “reality check” the BBC attempts to rebut seven of the “most frequently-shared” “false and misleading claims”.
It’s written by Jack Goodman, a “producer, newsreader and reporter at BBC Radio Derby”, and Flora Carmichael, a “journalist and producer with a strong track record of developing media partnerships and managing international projects and teams”.
So you can see why they would be well-qualified to set straight Oxford’s Professor Sunetra Gupta, Harvard’s Professor Martin Kulldorff, Stanford’s Professor Jay Bhattacharya and other eminent sceptics.
Let’s take each of the seven “myths” in turn.
1. “Here we are a year later – the world shut down for a 99.97% survival rate”
Verdict: This figure and similar figures being widely shared, are incorrect.
One recent estimate shows that overall, on average, about 99.3% of people who catch coronavirus survive it, according to statistics analysed by University of Cambridge.
That might not seem like a big difference, but it means that about 70 in 10,000 people are expected to die – not three in 10,000.
The death rate is much higher for older and more vulnerable people.
The “fact check” does not cite any sources for the claims it is debunking so it’s hard to know what the full context is. However, a search on Twitter brings up a number of recent tweets claiming that Covid has a 99.97% survival rate. While taken by itself this is not in line with current best estimates, a number of the tweets claim this is the survival rate once the over-65s have been vaccinated, though without citing a source. One tweet uses data from Minnesota to estimate a survival rate for the under-60s of 99.97%.
The BBC quotes 99.3% (IFR 0.7%) from the Cambridge MRC Biostatistics Unit, but it’s worth bearing mind that this is the same modelling team that produced the notorious projection of more than 4,000 deaths a day by the start of December, modelling which was already wrong on the day it was presented to the public by Witless and Unbalanced.
Professor John Ioannidis has estimated the global IFR for the WHO at 0.23% overall (survival rate 99.77%) and, for people under-70, 0.05% (survival rate 99.95%).
The BBC’s “fact-checked” IFR of 0.7% is therefore on the high side, and if the 99.97% claim refers to the under-60s (or to a scenario where all the over-60s have been vaccinated) then it would be within the ballpark of current data.
The wider point though is that the death rate has been greatly exaggerated, especially for those who are young and without underlying conditions. The median age of death with Covid is 83, and only 388 people under 60 with no underlying conditions died with Covid in English hospitals in 2020. Sweden, a country which did not implement strong restrictions (retail, hospitality and most schools remained open, there were no limits on private gatherings and no mask mandate) experienced only 1.5% excess age-adjusted mortality in 2020.
2. “Suicides increased ‘200%’ during lockdown”
Verdict: The only reliable recent data available on suicides in England – from the University of Manchester – has found that rates have not risen during lockdown.
Stay-at-home orders and the economic impact of the pandemic have undoubtedly taken a toll on people’s mental health. However, shared posts saying suicides have gone up by 200% during the pandemic are false.
It’s not clear where this statistic came from or who said it, but data on suicides is currently preliminary and incomplete. While 200% seems on the high side, mental health charities have certainly warned of a “second pandemic” of mental health problems and hospitals have said they are struggling to cope with the demand for children’s mental health services. According to a recent report in Irish News, suicide helpline volunteers in Dublin have doubled their hours to cope with surging demand during lockdown.
3. “Every winter hundreds a day die from respiratory diseases…’why are we locked down?’”
Verdict: Flu, a serious respiratory virus can be deadly – but there are vaccines and treatments available. Only very recently have vaccines for COVID-19 started to be rolled out, and only now are more effective treatments available.
The long-term effects of Covid can also be much more severe for many people and it’s more infectious than flu…
The risk of serious illness and death from coronavirus is significantly higher for older age groups.
While the pandemic phase of COVID-19 has been worse than a bad flu year in many places, it notably was not in Sweden, which suffered no excess deaths in 2019-2020 (July to July) despite going light on restrictions. COVID-19 is (or was prior to the population developing greater immunity to it) in many places one of the more deadly pandemic pathogens for older people in recent decades in the sense that it has claimed the lives of more older people than most previous pathogens. However, that is partly because of the older age profile of countries compared to pandemics in the past. Furthermore, the difference should not be exaggerated. The number of those who died from Covid, including in places which did not lock down such as Sweden, Florida (in the winter) and South Dakota, is only a very small percentage of the population. For instance, in South Dakota, which has not imposed any restrictions, only 0.22% of the population died with COVID-19 in the past 12 months, meaning 99.78% of the population survived the great pandemic year.
There are now numerous options for treatment and prophylaxis for COVID-19 that have been shown to be remarkably effective. They include (often taken in some combination) vitamin D, vitamin C, zinc, hydroxychloroquine, ivermectin, favipiravir, monoclonal antibodies and budesonide. In a number of cases, such as vitamin D and zinc, strong evidence of their effectiveness emerged early on.
4. “COVID-19 death rates have been falsely inflated”
Verdict: More than 125,000 Covid deaths have been recorded in the UK so far.
There are different ways of recording these deaths, but all broadly agree on the scale of the crisis.
About 90% of the deaths where Covid appeared on the death certificate had the virus as the underlying cause attributed by a doctor, according to the ONS.
The ONS total roughly matches up with Public Health England’s count, which looks at anyone who died within 28 days after a positive test, as well as the number of excess deaths, which is measured against a five-year average.
Almost all of these have been attributed to coronavirus, according to the UK’s three national statistics agencies.
All this “fact check” really shows is that all three UK statistics agencies have used a similar definition for a “Covid death”. However, there is certainly anecdotal evidence of widespread misattribution of deaths. A group of pathologists and medics have set up an audit to attempt to get to the truth of the matter. Consultant Pathologist Dr Clare Craig, who is leading the project, explains:
Many concerns about the coding of Covid deaths have been raised including:
– The side-lining of inquests.
– The deficiencies of tests.
– The alleged pressure on medical and care home staff to enter ‘Covid’ on certificates if a death has occurred within 28 days of a positive test.
This follows the publication of an article by Bel Mooney about the death of her father. Since then many similar cases have been recorded by Covid19 Assembly in which a loved one’s cause of death was recorded as ‘Covid’ although the deceased was never exposed to an outbreak, never showed any Covid symptoms and never tested positive to the virus. The Government has not responded to calls for a public enquiry.
Overseen by pathologist, Dr Clare Craig, the Covid19 Assembly team comprises experienced health professionals, researchers, data analysts and legal experts. They are now collecting evidence from medical staff, coroners, bereaved family members, registrars, funeral directors and mortuary staff. The aim is to ascertain to what extent (if any) official figures have been skewed by legislative changes to the registration of deaths.
One piece of data that is clear is that the Covid deaths peak was higher in winter, but the excess deaths peak was much higher in spring. That by itself is an indication that something is not right in how Covid deaths have been classified and the matter needs looking into further.
5. “No-lockdown Sweden fared better than the UK”
Verdict: It’s true that Sweden has had a lower Covid death rate than the UK, but it has fared significantly worse than its neighbours, all of which had tighter initial lockdown restrictions.
Many people opposed to Covid restrictions point to the example of Sweden, a country which at the beginning of the pandemic avoided introducing a compulsory lockdown, and instead issued voluntary distancing advice.
However, Sweden is a very different country to the UK and has characteristics that may have helped it during the pandemic.
It has a lower population density, and a high proportion of people live alone. The capital, Stockholm, is also less of an international transit hub than London.
When compared to other Scandinavian countries with similar population profiles, Sweden has fared much worse and recorded a significantly higher number of deaths than its neighbours, all of which have had tougher restrictions during much of the pandemic.
This “fact check” concedes the point in the first 14 words then spends the rest trying to minimise the importance of that with some version of the ‘neighbour argument‘. The truth is Sweden came out pretty average for a European country, and it is Norway and Finland (not so much Denmark anymore) which are outliers in terms of Covid cases and mortality, being unusually low.
Really, though, the neighbour argument misses the point. Lockdowns are sold to the public on the basis that without them you will see “hundreds of thousands of deaths”. That’s what all the models threaten and what seems to persuade people that There Is No Alternative. If, then, a country like Sweden (or a state like Florida or South Dakota) doesn’t lock down and doesn’t experience the threatened catastrophe then that invalidates the models and shows the threat is a false alarm. The inability or refusal of lockdowners to accept this basic point of empirical science is both mind-boggling and maddening.
6. “There was no pressure on the NHS all winter”
Verdict: Hospitals were very busy, particularly over the winter months, but the NHS has been able to cope, largely because of restructuring and lockdown restrictions.
The strain on critical-care beds has been acute, along with the specialist staffing required.
The number of adults in critical care was far higher than previous winters. In the last week of January 2021, some 2,000 more critical care beds a day were occupied in England compared with the previous year.
It seems clear that it was a particularly busy winter in intensive care this year, though it’s important to acknowledge that the NHS did cope (there was always spare capacity in the expanded provision), and the expensive Nightingale hospitals were barely used. A lot of additional pressure came from high staff absences due to constant PCR testing and the requirement for contacts to isolate. The claim that the health service coped because of “lockdown restrictions” is pure assertion as the hospital systems in Sweden, Florida and South Dakota also coped this winter and those places did not lock down.
7. “With PCR, if you do it well you can find almost anything in anybody”
The PCR (polymerase chain reaction) test is considered the most reliable way to detect coronavirus.
The process was invented in the 1990s, long before Covid appeared, by Californian scientist Kary Mullis. At a public event, he once said: “With PCR, if you do it well you can find almost anything in anybody.”
This has since been used to discredit PCR testing for Covid, but these criticisms are unfounded.
Mr Mullis was referring to the high level of sensitivity of his test.
PCR testing can pick up a tiny amount of virus, so it is possible for someone to get a positive result if they go for a test days or weeks after an infection and are not actually infectious any more.
However, this is unlikely to have a significant effect on the number of cases, and people tend to have a test when they have symptoms.
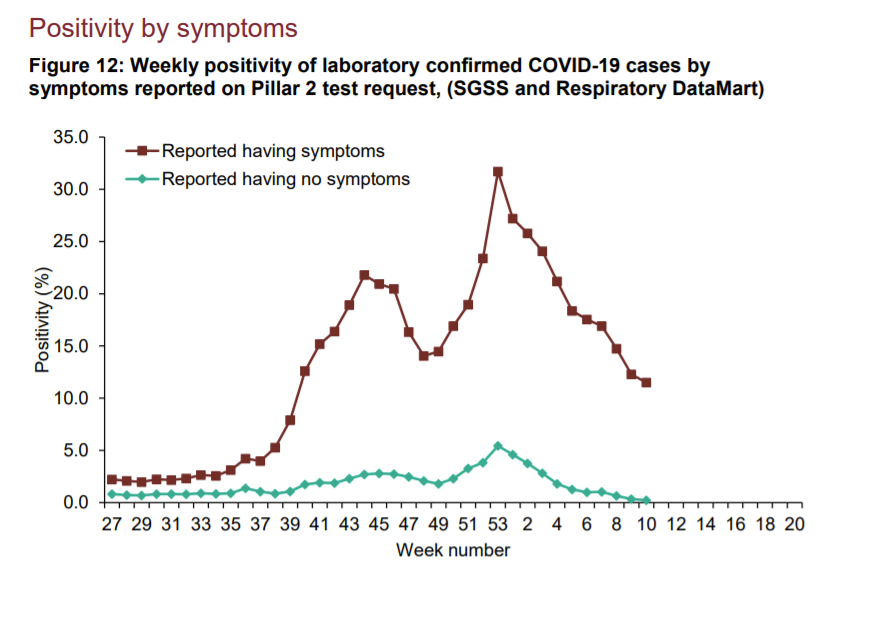
The “fact check” does not provide any sources for its claims that cold positives are “unlikely to have a significant effect on the number of cases” and that “people tend to have a test when they have symptoms”. In fact, about 12% of those who have symptoms and get tested are testing positive at the moment (see graph below), whereas overall positivity for Covid tests is around 2%. That suggests that the large majority of tests (around 89%) are being done on asymptomatic people.
Once again, the BBC has failed to recognise that when prevalence is low (as it is now) almost all positives are false positives as the true positives make up a smaller and smaller proportion of the total.