
NHS Hospital Pressure: The Ugly Truth
Mon 12:58 pm +01:00, 16 Nov 2020
This is the ugly truth about the winter 2020 Hospital pressure. #COVID is not the enemy of the NHS ??
? AN ESSENTIAL READ: This is a little too long for Facebook (1300 words, 5mins), but a must read in better understanding the NHS/COVID story.
WHAT IS COVERED:
?The alarmist messaging from Govt & NHS leadership
?The operational scale & reality of the NHS
?How NHS manage winter pressures & bed occupancy
?The impact of the virus & our initial response
?The enormous burden of the continued COVID-19 response on the NHS
? COVID-19 – the excuse and enabler for huge investments. Honesty and science has needed to be sacrificed…
? What can and should you do with this information?
PANIC STATIONS… APPARENTLY
The messaging has been intense and compelling… “an explosion in COVID-19 cases (positive tests) is straining the NHS, and hospitals will run out of beds due to COVID-19 unless public action isn’t taken”
We’ve had Dr Pittard, Sir Stevens and the Whitty-Vallance combo declaring a situation that is spiralling out of control, and that the NHS is 1-2 weeks away of running out of Hosp AND Nightingale capacity.
Well, since the 2nd pre-Lockdown fanfare, projections have quietly been revised down and alarm bells have stopped ringing.
Moreover, when you dig into Trust stats all over the country, COVID-related burden is mostly immaterial (excluding a small subset).
On the 12th Nov, NHS will release Trust-level detailed reporting on COVID & non-COVID activity, but generally we’ve had various insights in October showing seasonally normal patterns in the NHS.
So, WHAT’S ALL THE FUSS ABOUT?
THE OPERATIONAL REALITY OF THE NHS
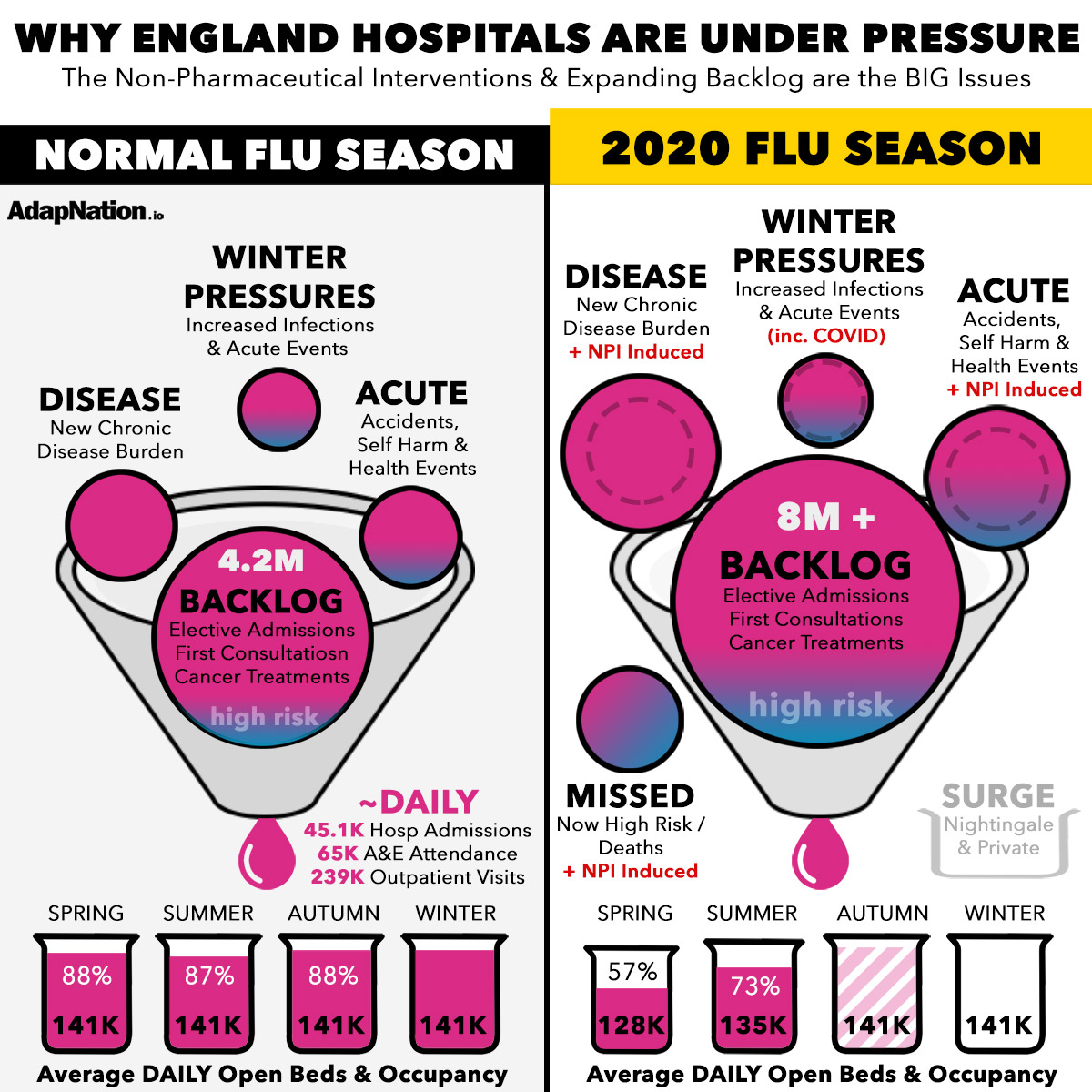
Study the graphic below. A lot going on, but it’s a straight forward yet worrying story.
There are 223 NHS Trusts in England, covering some 1,500 NHS hospitals by best estimates. There are about 1.1 million people employed in the NHS.
We’re talking big numbers – but it still isn’t enough to match the declining health of our population – principally due to having a disease care service, not a preventative healthcare offering.
On average, NHS Hospitals receive 45.1K hospital admissions EVERY DAY. Combine that with 65K A&E attendances and 239K Outpatient visits. Chronic diseases are spiralling out of control…
Plus we’re keeping people alive longer with conditions that need perpetual highly dependant care.
We have on average 141K beds available per day throughout the year, and we easily keep them occupied all year. NHS deliberately manage to ~88% occupancy overall – with a few Trusts running up to 92% due to their regions disease burden.
This is possible because of the sheer volume of people on the Waiting List for treatment (4M+ pre COVID), combined with a steady stream of people developing worsening conditions of diet and lifestyle.
These two factors alone could comfortably keep all hospitals at 100% capacity throughout the year. Even if we could double NHS capacity there would still be 90% utilised. So why are we not at max utilisation?
Well, it comes down to detailed operational management. Hospitals need to have capacity to serve acute care across A&E and many other wards. After all, this was the primary intention of hospitals, before chronic conditions exploded from the 1950’s.
BUSINESS AS USUAL WINTER NHS PLANNING
The cold weather, less sunshine and the resultant lifestyle and habit changes make the Autumn/Winter a particularly rough time for acute care.
But, the NHS know this.
They dial back on elective procedures, screenings, consultations etc to give the system extra headroom. If it’s panning out to be a soft winter, they dial up the elective stuff. If they see an above average spike in admissions, they pull back elective service.
The net result being that the NHS run at just under 90% year round, with more difficult decisions needed to be made in Autumn/Winter. They prioritise the most urgent and at risk elective services during this time.
It sounds like an operation nightmare to be honest.
And then, the year of COVID and the political obsession came…
THE VIRUS & OUR INITIAL RESPONSE
OK, so we’ve established the NHS was already drowning.
You can blame funding, and maybe that’s fair. The bigger issue is the declining metabolic health of our population as a result of a healthcare setup where there is zero personal accountability and consequence, nor any productive preventative measures from Govt.
So, when the COVID-19 Pandemic wave crashed over England, we were already up a creek without a paddle. Terrible population health, a soft prior winter, and a strained NHS is a bad combo.
Our response was to evacuate our Hospitals and close our books to elective procedures and service. Seemed fair to do so in March/April, but irrationality took over and the service has been intentionally been run lighter since.
We dropped capacity in spring, I guess due to closing of wards, COVID-19 wards, and social-distanced configurations. More surprisingly though, is that we had a record low in terms of occupancy – an average of 57%!
In the Summer, the NHS began its slow ascent up to more reasonable occupancy numbers, but still only operating at ~73% utilised. Intentional, but also a function of infection fears from patients and staff.
THE COVID-19 HANGOVER IS REAL
NOW, we have a real-world nightmare on our hands. Our Waiting List for surgeries and procedures has doubled, with estimates suggesting between 8-10 Million by the end of the year!
But it gets worse. Those procedures and surgeries missed have now increased in urgency and risk. The waiting list has accrued a greater number of higher risk patients that need prioritised service.
And, the Non-Pharmaceutical Interventions (Lockdowns, lack of exercise, isolation, reduced healthcare & screening) has resulted in an increase in disease progression and disease burden – i.e. more people now needed service.
And, The Acute care is expected to swell this winter too – more heart attacks, more mental health issues, more neuro-degeneration, more diabetes, more late stage cancer, and more self harm incidents etc.
AND THEN… then we get to the standard winter pressures of increased infectious disease and illness – with an increase of serious gastro and respiratory issues. Somewhere in that mix, we will see an Endemic burden of Coronaviruses, including SARS CoV2.
PLEASE UNDERSTAND this:
The NHS will NOT get overrun this Flu Season. Smart people will prevent that from happening. And, if we miraculously doubled our Hospital Capacity overnight, we would still be running at ~90%.
We have NO SHORTAGE OF PATIENTS….
COVID-19 – THE EXCUSE & ENABLER
Coronaviruses are real. We had an Epidemic in Europe between March-May. It was unavoidable – both the loss of life and the negative impact of the NHS and the economy.
But, and it’s a big but, Politics and healthcare/medicinal objectives have been in the driving seat. It’s not been about a genuine concern that there is an acute and sustained Public Health risk.
The NHS need huge investment. Not because of unfair treatment, but because of the increased disease burden imposed on them.
They have received £10’s of billions this year – directly and indirectly.
NHS leadership had a choice. Follow the science, or support the narrative in order to get enormous extra funding that will bring capacity, modernisation, extra staffing and a means to attempt not drown in backlog patients.
All, must I add, with naive overwhelming support from the people. No democratic public vote, no inspection by taxpayers on performance and investment requirements.
This is NOT lying, per se. Instead, it’s careful stretching and bending of the truth, and being very selective on what information is shared to the public.
WHAT TO DO WITH THIS INFO?
We cannot avoid the realities of the NHS situation. It unlikely serves us to push back on the NHS investments being made.
Locking down may help manage demand on the NHS a little, but not because of COVID-19. Instead, there will be justification to extend wait times push back on non-urgent care. Maybe there will be a few less accidents.
That said, the acute care derived from seasonal patterns of respiratory conditions will not be abated.
Moreover, we have seen a near doubling of attempted suicide, and we can expect increased heart, cancer, blood, brain and liver issues. We’re more ill than last year, and Lockdown will cause more NHS pressure, not less.
Things to consider for yourself:
- Understanding and improving your Metabolic Health
- Prioritise self care, nutrient density and exercise
- Help those around be less socially isolated
- Really dig into the research and assess the necessity of both the Flu and COVID-19 vaccine
- Don’t support and advocate the untruths regarding NHS COVID-19 overwhelm
- Think about if you want to be a COVID statistic as a result of voluntary non-symptomatic testing
#FactsNotFear
_____
SOURCES:
- NHS: Historical NHS Bed Availability & Occupancy
- BMA: NHS Missed & Cancelled Services April-August 2020
- THE WEEK: NHS Backlog Significantly Increases
- Detailed NHS Confederation Operating & Performance Statistics
- Kings Fund: Key Facts & Figures about the NHS
- NHS Confederation – the NHS Reset Programme, Sept 2020







