
Virus Crisis in France: Epidemic FINISHED vs. Organized Panic. Why?
Tue 9:48 am +01:00, 4 Aug 2020
ER Editor: We’re particularly interested in a highly informed perspective from France as France seems to ‘drink the koolaid’ longer than most countries, at least on the surface.
The article below is written by paediatric oncologist Dr. Nicole Delépine, who is not afraid to speak out on important issues. Her Twitter account is here, her website with orthopaedic surgeon and husband Dr. Gerard Delépine here. This is the first article we have found to summarize the French situation adequately, a summary which is disturbingly similar to everything we’ve published about government response to the covid plandemic in several countries. One can only believe there has been a massive and highly co-ordinated campaign coming from a very high place to control our governments’ policies.
Dr. Delepine exposes more of the medical criminality by the French government below, including the large doses of injectable clonazepam (Rivotril) it permitted for the elderly in medical difficulty, leading to suspicions of covert euthanasia.
********
Coronavirus Crisis in France: Epidemic Finished vs. Organized Panic. Why?
DR. NICOLE DELEPINE
In March 2020, we entered a delusional world governed by the fear and lies of our authorities, who are currently doing everything to prolong the panic without any real medical justification.
Lockdown: the worst French disaster since 1940
In March, our President declared war on Covid19, and his ministers explained to us that the suspension of fundamental freedoms, the obligation to “stay at home” (under tight police control) and the severing of all social ties were necessary to save our elderly, prevent our hospitals from being overwhelmed and limit the number of deaths that Covid would inevitably inflict on us. The President’s declaration of war on Covid is a clear sign that the United States is not going to be able to continue its war on Covid.
Three months later, we note that these measures led to the murder of our elderly in the Ehpads (ER: French carehomes), that the beds in private clinics remained empty even in the regions that recorded the highest number of Covid19-related hospitalizations (and transferred patients abroad), and that France is among the countries with the highest number of Covid19 deaths per million inhabitants.
The reality is the exact opposite of what was announced to us by the apocalypse preachers, their computer simulations [2] and the scientific committee, the same one that today recommends that we wear masks, get tested and install a tracking application on our phones (stop covid) when the disease has left our territory.
The assassination of our elderly
The protection of our elderly, designated Covid19 victims, was the “official” priority objective of the lockdown. However, all the measures taken during the emergency law resulted in eliminating them without witnesses, and preventing them from paying their last respects. The premeditated murder of Ehpad (care home) residents by untreated Covid and/or Rivotril is the saddest infamy of the lockdown.
The term assassination is violent, but corresponds to the recorded facts of an organized killing. The first step was to cut them off from their families, turning them into “prisoners in solitary confinement” [3], making them more vulnerable and facilitating slippage syndromes (progressive disinterest in life, rendered insipid by the absence of contact, leading to death) when it would have been possible to maintain protected contact. The second step was to prohibit them from diagnostic tests[4], then resuscitation[5], and then hospitalization. The third was to send sick residents back to their home institution or, in the absence of a real possibility of isolation, protective equipment and sufficient staff, they contaminated their fellow inmates. The final solution was the Rivotril decree[6] which organized the dispensation of a product intended to kill them on mere suspicion of Covid (without diagnostic certainty), with the drafting of a “preventive” order and the preparation of a nominal syringe without warning the patient or his family or even waiting for a possible aggravation. (ER: Rivotril is the commercial name for clonazepam, a sedative that is part of the controversial benzodiazepine family of drugs.) On 6 May 2020, dependent elderly people living in Ehpads accounted for half of the deaths attributed to the epidemic in France (12,769 deaths out of 25,531) [7].
The alleged objective of lockdown has therefore not been achieved at all, or even targeted.
Empty hospitals
During the containment, hundreds of thousands of people were unable to receive the care they needed because the White Plan reserved all hospital capacity for the COVID-19 tsunami, which “was bound to overwhelm us everywhere.”
In fact, many hospitals were left half empty throughout April, and the empty private clinics had to resort to short-time working for their staff. Thus, the private hospitalization union announced that a very large number of requests for short-time work had been filed in its establishments[8] and asked that the ARS (regional health agencies) refer to them the patients who could not be treated in public establishments[9]. 9] But with the exception of a few Parisian clinics and for a fortnight, the private beds remained empty for lack of patients.
During this period, in order to show that it was efficient, the government organized large TGV shows covid, Evasan [10] Covid and Covid military field hospitals, when it was sometimes enough to merely push open a door to find the beds, respirators and caretakers in sufficient numbers. In the Far East (ER: of France, near Germany, which had a lot of covid cases relatively speaking), on Wednesday 25 March, 150 resuscitation beds were available for Covid cases in public and private hospitals, with the possibility of creating 300 additional ICU beds. “Given the situation in the East, it is difficult to understand why these beds remain empty. All the more so as patients are being transferred to other regions“, said Pénélope De Feuquières [11], head of communications for the Elsan group, which has 120 establishments throughout France, mostly in the regions.
In this dramatic production, France is no exception: in Wales, of the 17 field hospitals that were set up to treat 6,000 COVID-19 patients, only one was used for 46 patients and today it is empty, too. The exercise cost £166 million [12]. In Lombardy, the most affected region in Italy, the COVID-19 Fiera di Milano hospital, which cost 20 million euros, only treated about 20 patients [13]. 13] Similarly in Madrid, where the huge field hospital was a disaster.
One of the world’s worst Covid19 mortality rates
A health measure is judged by its outcome: the number of deaths per million inhabitants. On this criterion, according to the WHO figures of 24 July, France ranks 6th in the world for the highest number of deaths among the 197 member states with 483 deaths/million behind Belgium (846/M), Great Britain (671/M), Spain (608/M), Italy (580/M) and Sweden (562). Best placed were Taiwan (1/M), Japan (8/M), Korea (6/M), Singapore (5/M), Malaysia (4/M), Morocco (8/M), Algeria (27/M), India (24/M) and malaria-endemic African countries whose populations take daily antimalarial drugs. (ER: this, of course, includes Hydroxychloroquine-related drugs)
If we had decided, like our German neighbours, to quarantine (isolate for 15 days) the virus carriers from the healthy population, we would have had 25,000 fewer Covid19 deaths. At the beginning of this epidemic, the Germans did not have more tests than we did for this new disease, but their Chancellor allowed all laboratories, including veterinarians, to carry out tests, whereas in France the Ministry and the Regional Health Agencies disregarded the offers made to them. Moreover, even without tests, the quarantine of infected patients would have been possible and effective on simple clinical signs because, contrary to what has long been claimed (and partly responsible for the errors of the crazy modelling that served as an alibi for our policies), asymptomatic infected persons very rarely participate in the spread of the disease [15]. 15] But health authorities preferred to send the infected without any sign of seriousness back home, and the elderly in Ehpads to infect their relatives thanks to the lockdown that increased the duration of exposure to the virus.
Tens of thousands of collateral victims
The “white plan” activated during the state of emergency and the blind lockdown adopted led to the cessation of treatment of chronic diseases (hypertension, diabetes, cancer), a source of significant loss of chance to survive. It also blocked the diagnosis and treatment of new infectious pathologies, cancers, etc. that appeared during the lockdown and remained progressive in the absence of diagnosis and treatment. Even modest delays in cancer surgery have a significant impact on survival. To the direct victims of Covid19 and containment, the White Plan therefore added collateral victims through discontinuation or delay of chronic disease care and delays in diagnosis of previously ignored diseases.
In a report[16] F. Bizard states: “the CNAMTS has confirmed a 40% drop in activity for general practitioners. An average of 70% loss of surgical activity has been observed since the beginning of the white plan.:
The impact of the Covid-19 crisis has been estimated at a decrease of more than 2 million surgical procedures, for a lifting date of the white plan after June 1. Ongoing treatments for known cancers have been delayed or modified. LRAs have even suggested treating known colorectal and lung cancers with radiotherapy, even though such treatment is significantly less effective than surgery and overburdened radiotherapy departments often make appointments in two months or more.
Call from doctors and surgeons for the lifting of the White Plan
The Academy of Medicine[17], the BLOC[18] and other representatives of surgeons in France have sent warnings to the highest authorities of the State.
“We are witnessing every day and more and more the aggravation of morbidity and mortality of non COVID patients. Patients are presenting aggravated conditions with diagnostic and therapeutic delays with serious consequences. All medical specialties are concerned. Enacted to combat the COVID19 risk, the White Plan now has deleterious effects on public health, even though the epidemic is almost extinct over a large part of the country. Its risk/benefit ratio has become catastrophic”. To no avail.
Since the lockdown, in three months, 90,000 new cancers should have been diagnosed and treated, but most of them were not. While for years, the National Cancer Institute, the High Authority of Health and the league against cancer have been constantly reminding us of the crucial importance of early treatment “the earlier a cancer is detected, the greater the chances of cure” and that they constantly advocate all cancer screening.
The epidemic evil of government decisions: the White Plan equivalent in Great Britain
Our English neighbours have estimated the health impact of the cessation of medical cancer activities in Great Britain. Professor Turnbull’s team [19] [20] calculated that if the 94,912 patients – who had to undergo surgery to remove their cancer – were three months late, there would be 4,755 additional deaths over the next five years. Given the expected lifespan of patients after surgery, the delay would represent 92,214 years of life lost.
“To avoid a public health crisis related to preventable cancer deaths, cancer diagnosis and surgery must be maintained at their normal pace, with prompt attention to any backlog that has already accumulated.”
During the same period, more than half of digestive, cardiac[21], vascular, neurological, rheumatological, psychiatric and pulmonary diseases were not seen in consultation, and worsened due to lack of timely treatment.
The number of deaths secondary to delays in care as a result of this white plan is difficult to count for the moment, but the considerable number of patients concerned (several million) raises fears that it could very well exceed the number of direct victims of the epidemic.
Heavy social consequences of indiscriminate lockdown
While there is no evidence that the tidal wave announced on the hospitals was prevented by the lockdown [22] [23], the measures ordered by the government have put whole sections of society in distress:
- youth deprived of their right to education
- progressive disinterest in work among many wage earners who are finding it very difficult to resume their activities
- heavily burdened public finances
- old people’s homes transformed into prisons while …
- the bonds among the population have been strained, undermined by mistrust and fear of the other.
- economic recession, worsening unemployment and misery are already being felt
The measures taken in the name of protecting the population were clearly neither effective, proportionate nor adequate.
In France, the epidemic is over
A disease exists when it results in sick people, people who show clinical signs, require care, hospitalization and are threatened with death.
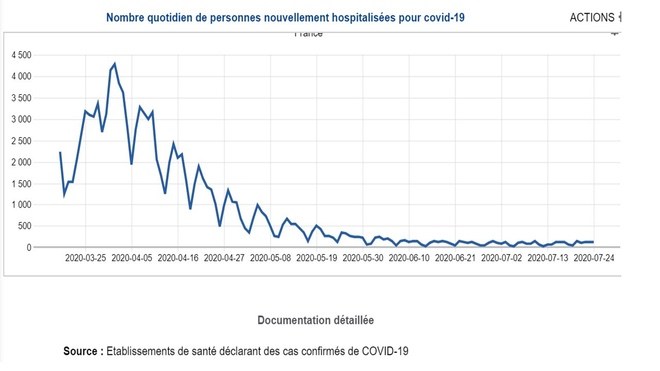
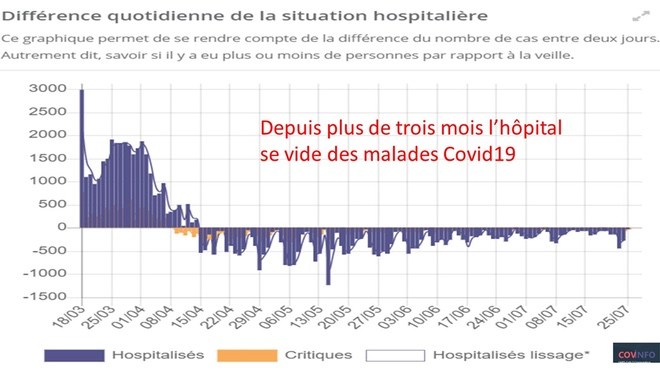
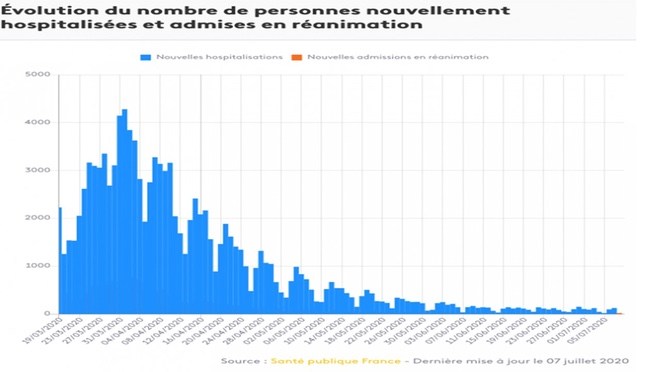
However, when consulting the official data of Public Health France, a continuous decrease in the number of hospitalisations, the number of people admitted to intensive care units and the number of deaths has been observed over the last 3 months.
These are key indicators of an evolving epidemic, as shown in the following official graphs:
“Daily number of people hospitalized for COVID-19”
“Daily difference in the hospital situation”
“Evolution of the number of people hospitalized and admitted into emergency care”
Since the beginning of the year, mortality has exceeded the upper limit of the statistically expected value only in the 65+ age category and only between the third week of March and the third week of April.
In the 0-64 age group, on the other hand, at no time did mortality deviate significantly from the usual values.
Epidemic over, but fear propaganda intensified!
Instead of highlighting this good news, the government continues its terror propaganda, under the pretext that the number of positive cases is increasing, even though this mainly reflects the sharp increase in the number of tests carried out.
When looking at the graphs showing the number of positive tests relative to the number of negative tests, it almost takes a magnifying glass to see the share of positive tests – which is otherwise stable, fluctuating since mid-May at around 1%.
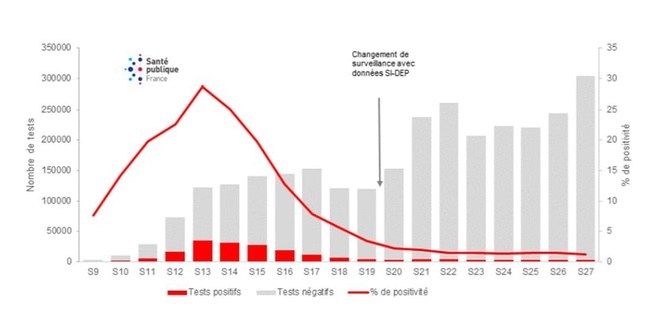
These positive cases are more likely to be false positives. The PCR tests currently in use have a margin of error of 1.8%. This means that out of 10,000 tests, there will be 180 false positives. However, since May 11, the percentage of positive tests has remained stable at 1%. With such low figures, the possibility of frequent false positives cannot be ruled out. In an analysis published in mid-June, *Beda Stadler, Professor Emeritus and former Director of the Institute of Virology and Immunology at the University of Bern, also pointed out that a large proportion of these “cases of infection” could in fact be people who are already immune to the virus and still carry “viral debris” in their bodies.
*ER: See the article we published by Dr. Stadler, titled Coronavirus: Why everyone was wrong.
The continuation of the propaganda of fear is effective, as shown by the number of consultations for covid19 anxiety, which Santé Publique France then uses to make people believe in a second wave:
“as a sign of a possible resurgence of the disease, from 29 June to 5 July, 1,523 medical acts for suspicion of Covid-19 were recorded by the associations SOS Médecins. This represents an increase of 41% compared to the previous week”.
Thus, despite objective and reassuring indications, adults of all age groups, and even children [24], are afraid of being contaminated, falling ill and dying from Covid-19. This unfounded fear raises the question of the responsibility of those who spread it and continue to perpetuate it. Psychiatric consultations continue to multiply, as does the need for hospitalizations that the services cannot provide[25].
What could be the reasons for such misinformation?
Why are the reassuring data available today not making the headlines? What is the point of imposing the mask when the disease has left the country, of making small children believe that they should not kiss their grandparents to protect them, of constantly reminding the public that the restrictions could be reimposed very soon if not to maintain panic and ensure the submission of the population?
Several reasons support this hypothesis.
Firstly, there is the inconsistency in the measures in place (most of which lack a sound scientific basis) and the way in which the behaviour of inhabitants is analysed by experts and the media.
Citizens who question the real current medical interest of masks, tests and tracing are labelled as irresponsible and are threatening public health and promoting a second wave. Here, it is the behaviour of people who massively celebrated the return of a little freedom and music that is being criminalized, while no increase in the number of sick people has been noted since these festive events. At the same time, the media were not moved by the thousands of demonstrators who invaded the streets of major cities at the same time to protest against racism, nor by the consumers who rushed to the sales as soon as the shopping centres reopened.
In the ranks of politicians and journalists, no one seems surprised at the major shift in the objective of the measures imposed from “flattening the curve” to “eradicating Sars Cov-2”, an undertaking that no scientist can deem credible.
This hypothesis is also given credibility by the similarity of this illogical propaganda of the rulers in many countries that the disease has deserted, such as Switzerland or Canada.
In a democracy, it is the people who must govern…
It is worth questioning the growing role that the members of the scientific committee and the executive are taking on themselves.
It should be remembered that this group of experts – too closely linked to the drug companies – is to advise the president and the defence council on the basis of its scientific knowledge. Not to govern in the place of elected authorities, nor to torpedo their decisions by issuing warnings to the public. Yet that is what these researchers have done by imposing stupid restrictions without any real health justification, making it very difficult for the president to reopen schools as he wants. This way of authorizing a group of unelected experts with little competence in clinical medicine and whose members were recruited on the basis of opaque criteria shows a bewildering lack of knowledge and contempt for democratic institutions, to say the least, and once again casts doubt on the capacity of the media to nourish democratic debate.
Virus Crisis in France: Epidemic FINISHED vs. Organized Panic. Why?







