
LOKIN-20: The Lockdown Regime Causes Increasing Health Concerns
Tue 11:24 am +01:00, 2 Jun 2020
ER Editor: One is left to assume from this carefully documented report that a) privatization of healthcare services, in this case for the elderly in their homes, is a dreadful idea for quality patient care; and far more consequentially, b) the government is complicit because of its policies (not just the lockdown policy, but that relating to not sending them to hospital) in relation to covid in at least some of the deaths of the elderly in care homes.
Add to that widespread reports of the Do Not Resuscitate notices, even prearranged by doctors’ offices for elderly patients who are not in care homes, and that otherwise empty hospitals have not been accepting elderly patients (as well as the non-elderly) who need regular care for other serious conditions. We really are left to wonder if this virus outbreak has not been used to cull the elderly, the ‘useless eaters’. The infamous Liverpool Care Pathway, ostensibly stopped, was the precedent-setter.
If we also take into account the rather stark reduction in life expectancy as a result of poverty (mentioned at the end of this article), you have to further wonder about the entire social engineering agenda behind the unnecessary lockdown policy of our governments.
********
LOKIN-20: The Lockdown Regime Causes Increasing Health Concerns
IAIN DAVIS
A new public health crisis, very recently identified as LOKIN-20, is raising increasing health concerns in the UK.
In their response to a respiratory illness called COVID-19 (C19) the UK State are among those who have responded by locking up their populations and destroying their own national economy. This appears to be causing LOKIN-20.
The most recent statistics from UK’s Office of National Statistics (ONS) raise significant concerns about health impact of the lockdown regimes favoured by some, but not all, governments. All in response to a disease which researchers at the Centre for Evidence-Based Medicine at Oxford University estimate to have an infection fatality rate (IFR) of between 0.1% and 0.36%. Similar to seasonal flu.
Of course, a syndrome called LOKIN-20 hasn’t been identified as a cause of death. However, in light of the current data, this post asks if it should.
LOKIN-20 AND THE LACK OF SCIENTIFIC JUSTIFICATION
Both Public Health England (PHE) and the Advisory Committee on Dangerous Pathogens (ACDP) were satisfied that COVID-19 (C19) presented a “low risk” of mortality and downgraded it from the status of a High Consequence Infectious Disease (HCID) on March 19th. The ACDP board members include Professor Neil Ferguson from Imperial College. Presumably Prof. Ferguson was among the dissenting voices on the ACDP board as he completely ignored the majority opinion of his scientific colleagues.

He said that infection rates of 60% of the population with a 1% mortality rate were possible. Standing by his prediction of 400,000 C19 deaths in the UK. The Imperial College computer model report was released to the public on 16th March, predicting huge numbers of deaths from C19. By the 19th March Prof. Ferguson must have known a majority of his peers disagreed with him.
When it comes to wildly inaccurate predictions, Prof. Ferguson’s work at Imperial College has a long and distinguished history. In 2002, he said that 50,000 people in the UK would die from “mad cow disease”: to date less than 200 have passed away. He predicted 200 million global deaths from the H5N1 bird flu: currently it is a suspected factor in the deaths of 455 people world wide. In 2009 he told the UK Government that 65,000 could die from swine flu in the UK and worked with the World Health Organisation to predict millions of deaths from the H1N1 global flu pandemic.
Suspected resultant UK deaths from swine flu were estimated to be 457 and the global total showed 18,500 laboratory-confirmed deaths from the H1N1 pandemic. The U.S. Center For Disease Control (CDC) claim there were many more, though their estimate varies between 150,000 and 500,000.
Quite an error margin and still considerably less than Imperial College’s fantasy. The CDC is heavily funded by flu vaccine manufacturers.
While Prof. Ferguson and his Imperial College colleagues have been consistently wrong, they have also been unquestioningly believed by governments and intergovernmental bodies on every occasion. Seemingly without reservation.
Despite the clear evidence to the contrary, policy makers from all political parties have shown tremendous loyalty to Imperial College’s silly data models. In doing so, they have not only ignored the researchers woeful history of failed predictions but have also denied the scientific evidence which usually contradicts them.
In no way can basing policy decisions on Imperial Colleges computer models be considered science led decision making. Quite the opposite.
LOKIN-20 AND LOCKDOWN MADNESS
Farr’s Law is observed with all viral diseases and describes the rate at which a viral infection increases and then declines in a given population. Initially, the virus has practically unlimited hosts and the rate of increasing infection is exponential.
As more people become infected, that rate declines. The numbers still increase, but the rate of that increase drops sharply. Once the rate starts to decline, virologists and epidemiologists can then predict the scale of the outbreak with some confidence.
It indicates that the disease has passed its peak potential and will wane naturally in the coming days and weeks. Regardless of intervention.
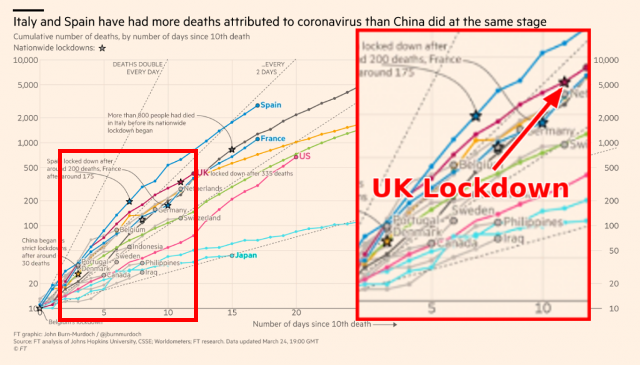
Increase in Mortality Analysis by John Hopkin’s University shown by The Financial Times
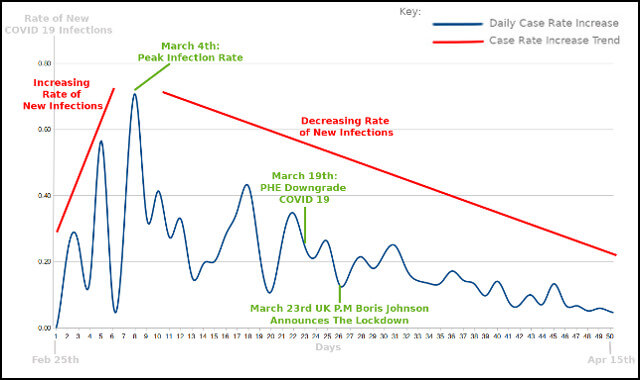
Based upon UK statistics released by Worldometer, we can see this initial rapidly increasing rate of infection and identify when that rate began to slow down. For the 50 day inclusive period between the February 25th until April 15th, this changing rate of increase was evident.
That rate peaked on March 4th and has declined since. Following the drop in this rate on the 4th, with a consistent downward trend to March 16th, the scientists on the ACDP board could predict the trajectory of the disease with some certainty and consequently downgraded C19 due to low mortality rates.
Calculating the daily rate of increase can be done simply by dividing the current day’s total number of cases by the previous day’s total. For example, on March 3rd there were 51 total cases rising by 36, to reach a total of 87, by March 4th. A ratio rate increase of 0.71.
This was the peak rate of increasing infections in the UK. From this date onward, the rate of increase declined markedly, in accordance with Farr’s Law. We can plot these figures to find the changing rate of the increase in cases.
This slowing rate of new infections is also evident when we look at the logarithmic scale of UK Infections rates. This produces the familiar infection rate curve synonymous with Farr’s Law.
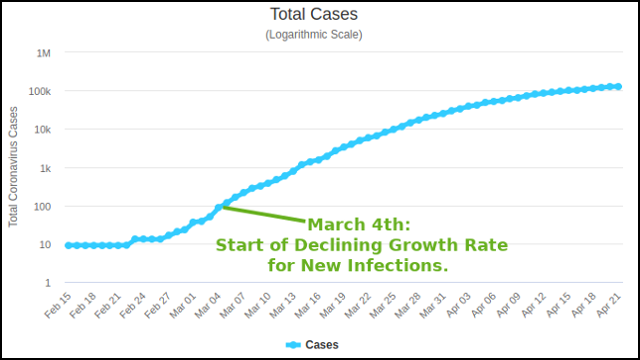
UK Case Infection Growth Rate From Worldometer
The UK government are among the many who apparently ignored the most basic concepts in virology and chose instead to base their lockdown regime upon the fictitious Imperial College models. All the science indicated that existing measures, encouraging the public to observe basic hygiene and limit interactions with vulnerable people, was working, as C19 followed the normal bell curve of any viral disease in a population.
There was no scientific justification for the lockdown. Nothing about the UK State’s response was “led by the science.”
Nor is there any evidence that lockdown regimes have any positive impact upon infections rates. Comparisons between severe lockdown states and those who opted for less draconian measures reveal no advantage to placing your population under house arrest.
States who chosen not to rip their economies apart appear to have fared much better. Sweden did not deploy a lockdown and yet, according to data from John Hopkin’s University, case rates per million of populations are lower.

Further comparative analysis supports these findings. In terms of limiting infection rates, there is no discernible benefit to lockdown regimes. In fact, Oxford University found a direct correlation between infection rates and the relative severity of lockdown regimes. It suggests the more stringent the lockdown, the higher the infection rate.

This is not unexpected, as numerous epidemiological studies have shown that infection rates for C19 are higher when people are exposed to it for prolonged periods in confined spaces. Locking people up in their homes is probably the worst thing you could do if you wanted to reduce the infections and the duration of the outbreak.
This is well known to the World Health Organisation. In their joint study with Chinese authorities, published in February, the WHO stated that airborne spread wasn’t reported for C19 and was not considered to be a method of transmission.
They found that most infections occurred within families where the chance of infection was as high as 20%. However, the chance of infection in the community was estimated to be between 1-5%.
The WHO also stated that COVID 19 is less virulent than influenza. They say it is spread by droplets and cannot linger in the air. Equally there is little evidence that flu transmission is airborne. The comparison between C19 and influenza is worth considering as we discuss LOKIN 20.
LOKIN-20 LURKS BEHIND THE DATA
About the only consistent element of the narrative we have been given about C19 is that we must believe the death toll is horrendous. This “alarmism” has been spread by State officials and the mainstream media (MSM). It is unmitigated drivel.
Here are some important factors to bear in mind whenever the MSM give you statistics about alleged deaths from C19 in the UK. These factors are unique to C19.
The ONS recording system was changed by the State, but only for C19, from recording only registered deaths to adding in provisional deaths assumed to be from C19. The RT-PCR test for C19 does not appear to be very reliable. Furthermore, the man who won the Nobel Prize for designing it specifically stated that it could not identify a virus. As previously stated, emerging studies indicate a much higher infection and thus much lower mortality rate for C19.
However, in the UK, a positive test is not even required for someone to be deemed to have died from C19. Nor does there need to be any clear evidence of causality for C19 to be declared as the underlying cause of death.
Merely “mentioning” C19 is considered sufficient. Regardless of other, often multiple, comorbidities and infections. In addition, from an age demographic perspective, C19 deaths appear to be indistinguishable from quite normal mortality.
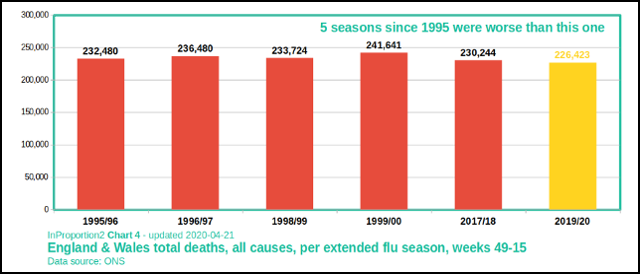
The Office of National Statistics (ONS) have reported a consistent rise in mortality between weeks 11 – 15, covering the period 7th March to 10th April 2020 in England and Wales. During that period deaths from all causes (all cause mortality) have steadily climbed and have been above the ONS 5 year average in weeks 14 and 15.
The ONS calculate the mean average from the 5 preceding years’ completed statistics. This means that any year prior to 2014, many with much higher than average mortality, are not used to calculate the current average.
There is no evidence that this year’s all cause mortality in England and Wales is in any way unprecedented. In recent history, 1995, 1996, 1998, 1999 and 2017 have all been years with comparable, if not higher, mortality. None were deemed reason to force the population to incarcerate themselves.
The demographics of the UK show a growing but ageing population. Age is the primary corollary for normal mortality and C19 is no different. The ONS expect the 5 year average figure to steadily increase while the population continues to age.
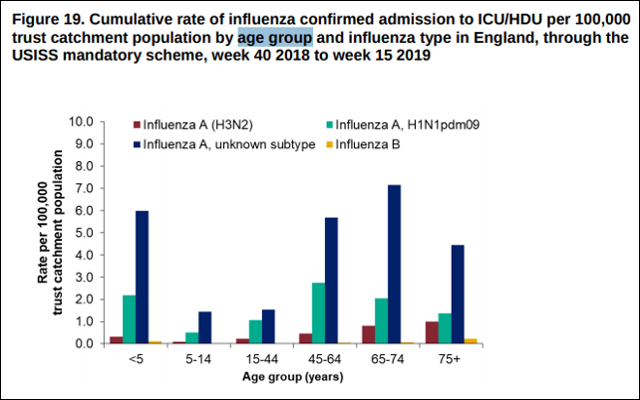
The MSM regularly report C19 suspected deaths among the relatively young. This is to give you the impression that C19 can strike anyone at anytime.
What they consistently fail to mention is that PHE records of ICU admissions for influenza indicate all ages are at risk from the flu. This is not the case with C19. Its risks apparently increase with age.
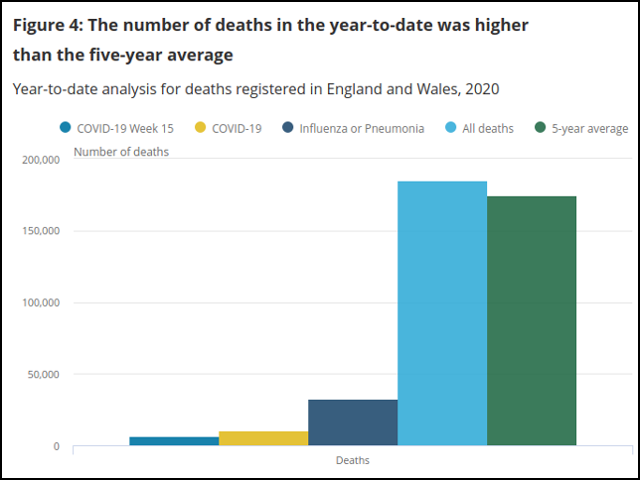
There was a media frenzy when the ONS released their all cause mortality statistics for Week 15.
This showed there were 7,996 deaths over and above the 5 year average. In total, 6,213 mentioned C19. Despite the MSM’s attempt to convince you this somehow proves C19 is a modern day plague, a cursory look at the data demonstrates that it is no such thing.
The ONS noted that these were the highest single-week mortality figures for England and Wales since 2000. This is true; however, the historical data also demonstrates that the one-week statistical record was exceeded in 2000, 1999 and 1997. Bluntly, not only is there nothing unprecedented about the overall mortality figures, the high one week spike isn’t anything new either.

To further put this into perspective, the population of England and Wales in 2000 was just under 53 million. In 2020 it conservatively stands at more than 60 million. That’s more than a 13% increase in 20 years, with a notable ageing of the population over the same period.
Normalising for population growth alone, irrespective of ageing, if 20,566 died in one week in 2000, then week 15 mortality figures in 2020 are equivalent to 16,109. About 4,450 fewer than in 2000, in relative terms. If we take similar normalisation into account for previous years of high mortality (1995, 1996, 1998, 199), then, as a percentage of population, relative 2020 mortality statistics are well below those years and further below 2017.
As the death rate from C19 reduces in the UK, it is clear that the C19 threat level never warranted the lockdown regime and the collapse of the economy. At the risk of being accused of heresy, it is absolutely possible to state that C19 is like the flu in many respects.

UK Statistics from Worldometer
LOKIN-20 SEEN IN THE DATA
As usual, in their week 15 report, the ONS noted what appeared to be a deliberate attempt to inflate the C19 mortality statistics. Of the 6,213 reported C19 deaths for week 15 in England and Wales, 2,333 also mentioned both influenza and pneumonia. It is impossible to see how these deaths can legitimately be called C19 deaths.
Consequently, all that can be said is that of the 7,996 excess deaths, beyond the 5-year average, 3,880 deaths mentioned C19 on its own, though we know from previous releases that more than 90% of those had at least one other serious comorbidity. The remaining 4,116 deaths were also attributable to at least one other infection and additional comorbidities.
The confusion about causes of death has been highlighted by the Royal College of Pathologists, who have called for a systemic review. The Health Service Journal reported that there was “uncertainty” about reported C19 deaths, and questions remained about how many may have died as a “knock on” consequence of the lockdown.
The reason for scepticism becomes clearer when we look at comparative death in the first 15 weeks of 2020. This shows considerably higher numbers of deaths from respiratory infections other than C19 in England and Wales.
When we also consider that attribution of C19 deaths are uniquely vague, and that a considerable proportion may well be attributable to influenza or other respiratory infections, the MSM’s insistence that C19 is the only story doesn’t stack up. Something else is happening too.
ONS reported all cause mortality 2020 to date
Frankly, we have no idea how many people have actually died from C19. Nor does the UK State.
Speaking on the 18th March the UK’s Chief Scientific Officer, former GlaxoSmithKline head of research and development, Sir Patrick Valance, clarified the situation for the British people. He stated:
It is worth remembering again that the ONS rates are people who’ve got COVID on their death certificates. It doesn’t mean they were necessarily infected because many of them haven’t been tested. So we just need to understand the difference.”
The difference appears to be that the C19 is the first disease in history from which you can officially die without any firm evidence that you actually had it.
The symptoms of C19 are very hard to distinguish from symptoms of other respiratory infections, such as influenza and the common cold. Diagnoses from symptoms alone seems even more unreliable than the RT-PCR test. Yet the ONS confirmed this is how C19 can be identified as a cause of death:
A doctor can certify the involvement of COVID-19 based on symptoms and clinical findings – a positive test result is not required.”
This is a consequence of the State’s advice to doctors which informs them:
if before death the patient had symptoms typical of COVID 19 infection….it would be satisfactory to give ‘COVID-19’ as the cause of death.”
As recorded C19 mortality shows a decline, once again, the state is changing the way statistics are recorded. It has now asked the Care Quality Commission (CQC) to record more suspected cases from social care settings. Speaking on the April 14th a CQC spokesperson reportedly said:
From this week, the death notifications we collect from providers will allow them to report whether the death was of a person with suspected or confirmed Covid-19.”
 If the system for recording hospital C19 deaths is questionable, the one suggested by the CQC for care homes is downright bizarre. At the request of the State, the CQC have asked non medically trained care home providers to report, what they suspect, are C19 cases. These figures will then be added to the claimed C19 mortality figures.
If the system for recording hospital C19 deaths is questionable, the one suggested by the CQC for care homes is downright bizarre. At the request of the State, the CQC have asked non medically trained care home providers to report, what they suspect, are C19 cases. These figures will then be added to the claimed C19 mortality figures.
The lack of testing in care settings suggest the CQC will be adding far more suspected cases to the ONS statistics than confirmed. Care homes other than nursing homes do not typically retain medically trained staff. The vast majority of those who suspect C19 from care homes won’t be basing their suspicions on qualified medical opinions.
The claimed C19 mortality figures are so disparate they have become practically worthless from a statistical perspective. Even if we accept all reported C19 deaths resulted from it, which is a very long stretch, clearly something else is also pushing up excess mortality in England and Wales.
Over the two week period of weeks 14 and 15, of the 14,078 additional deaths, 8189 people lost their lives due to something other than just C19. We don’t yet know what other factors may be playing a part in the increase. All we can say is that excess mortality was unusually high and, at most, plausibly claimed C19 deaths accounted for less than 42% of those deaths.
So what other changes may have impacted mortality this year? One in particular stands out. The lockdown itself.
Are we starting to see the consequences? Could we call this LOKIN-20?
The evidence strongly suggests that possibility.
LOKIN-20 DISPROPORTIONATELY AFFECTS THE MOST VULNERABLE
LOKIN-20 appears to be the increased health risk caused by the lockdown regime. Those most at risk from LOKIN-20 are the same people who are at highest risk from C19. This additional “wave” of mortality, as a direct consequence of the lockdown, has recently been highlighted by NHS data analysts Edge Health.
Based upon ONS weekly figures, their comparative analysis of excess mortality and A&E attendance highlighted the significant impact of LOKIN-20. Speaking of an initial second and then third wave of mortality, from the impact of the lockdown, the co-founder of Edge Health George Batchelor said:
“If projected forwards, these numbers get so large it is hard to relate to them on a personal level. Unlike the current peaks, this third wave may be spread out over a longer period of time. But make no mistake this could be could be a very deadly wave.”

Edge Health Analysis
Those who require home care, vulnerable adults in care settings and older people in care homes have been all but abandoned by the State. This is a direct result of its counterproductive lockdown regime. Dying from systemic neglect appears to be a symptom of LOKIN-20.
During the alleged response to the C19 pandemic, you might imagine the State would streamline vulnerable people’s access to potentially lifesaving medical interventions. However, it has done the precise opposite.
Spreading disinformation, the MSM reported that there were 7,500 C19 deaths in care homes in weeks 14 and 15. This was fake news.
Of the 7,500 excess care home deaths, only 1,500 were attributed to C19. Analysis by the Health Service Journal (HSJ) found that 80% of these people probably died from something else.
They identified 6,000 people, without diagnosed C19, who had died in care or at home. Were it not for the lockdown, these people would otherwise have gone to hospital.
The HSJ assumed these people would have died anyway, and they may well be right. But who knows how many would still be with us had they received the hospital care they needed.
This appears to be just one of the health consequences of the State’s lockdown regime. It seems to be precipitating vulnerable people’s deaths in a variety of ways.
 During the same period the NHS issued guidance which stated care home residents should not be conveyed to hospital. At the same time, ambulance response times increased dramatically. Being unable to get emergency medical support when you need it is another apparent LOKIN-20 symptom.
During the same period the NHS issued guidance which stated care home residents should not be conveyed to hospital. At the same time, ambulance response times increased dramatically. Being unable to get emergency medical support when you need it is another apparent LOKIN-20 symptom.
Rather than more closely monitoring care homes and isolating vulnerable people from infection, the State decided not to bother. The care industry has been calling for widespread testing and Personal Protective Equipment (PPE) since the start of the outbreak. So far neither the testing nor the PPE has materialised.
There is currently considerable capacity within the NHS for the people dying in care homes to be treated in hospital. The State continues to build Nightingale Hospitals across the country, most of which are completely empty . While we are misled into believing people are dying in their many thousands in care homes from C19, it appears most are dying from a lack of treatment from every condition other than C19.
Instead of providing medical treatment, there are widespread reports of residents having “do not attempt resuscitation” (DNAR) notices attached to their care plans by visiting NHS practitioners. Other more vulnerable adults, such as those with learning difficulties, who frequently have additional comorbidities, are also effectively being told to drop dead.
The UK’s home care industry, providing care to older people living in their own homes, warns that many providers are unable to cope with the additional costs imposed upon them by the lockdown regime.
Raina Summerson, the chief executive of one of England’s largest home care provider Agincare said:
“With a lack of funding and sky-high costs of PPE, there will be providers who go bust….Overnight, local authorities will have the responsibility of picking up care for bankrupt providers but will not have resources to do so. It could well mean people left without care and, in the worst-case scenarios, falling through the cracks and dying alone at home.”
The UK Health Secretary Matt Hancock recently made the magnanimous gesture of allowing families to see their loved ones who were dying of C19 in care homes. Whether that offer extends to the families of the majority who are seemingly dying from a lack of medical treatment isn’t clear.
Meanwhile, under his watch, either by design or rank ineptitude, the UK State has effectively created what appears to be a euthanasia program. His platitudes are grotesque.
LOKIN-20 IS EVERYWHERE
Accident and Emergency attendance has dropped to a record low while the percentage of admissions following attendance have risen to a record high. This means people are presenting to A&E for suspected C19 but little else. However, given the dramatic increase in ambulance response times, perhaps many are simply not making it to A&E alive.
Dr Katherine Henderson, the President of the Royal College of Emergency Medicine, stated:
We are concerned that this drop in attendance may mean that people with serious health problems are avoiding going to their emergency department for fear of getting coronavirus….Even before Covid-19, we knew that patients were getting sicker – people are living longer and acquiring more health problems……The most important thing the public can do at the moment is to stay indoors and follow the government’s advice…..But do seek medical help if you need it – don’t stay at home with a heart attack out of fear.”

Dr Katherine Henderson
I think we can all agree that the State and the MSM have ramped up fear of C19 to quite extraordinary levels. As we have discussed, the medical and scientific justification for this is largely absent. The propaganda seems primarily designed to justify the lockdown regime.
It is absurd for the State and senior health professionals to now express concern that people aren’t going to hospital when they need to. Of course they aren’t.
To claim this was unforeseen is ridiculous. The whole UK propaganda narrative has urged people both to be terrified of a flu-like illness and stay away from health services to “protect the NHS.” The first annual increase in coronary heart disease mortality in the UK, following nearly two decades of steady reductions in the UK, was noted last year, before LOKIN-20 began.
The former president of the Society for Acute Medicine Dr Nick Scriven stated:
“The biggest fear is people sitting at home ill and not attending A&E […] people feeling sick at home or having a heart attack and not coming to hospital as they are frightened…We have seen a few sick young people just sitting at home for five or six days getting worse and worse”.
The president of the British Cardiovascular Society Simon Ray stated:
“It seems there has been a uniform reduction in hospital attendances for heart attacks…..it’s around 40% down in terms of callouts for emergency treatment for heart attacks….There also seems to be substantial reduction in referrals in for acute coronary syndrome….A number of units have also reported people presenting late with complications due to having a heart attack that we don’t normally see. The concern is people sitting out symptoms rather than calling help.”
It is clear, people with acute need for cardiovascular treatment are not presenting to hospital as they otherwise would. Fear driven reluctance to access health services, when they are most needed, appears to be another symptom of LOKIN-20.
Around 170,000 people die every year from cardiovascular disease in the UK. A 40% reduction in callouts present a potential health crisis which dwarfs any perceived risk from C19.
This is entirely due to the lockdown. Part of what we might call the LOKIN-20 condition.
There is no “surge” in C19 patients and there are more empty hospital beds than ever before. Yet the risk to cancer patients from withheld treatment has increased significantly during the same period. Thanks to LOKIN-20.
This prompted Gordon Wishart, Professor of Cancer Surgery at Anglia Ruskin School of Medicine, to write to State officials urging the rapid reestablishment of access to screening and treatment for cancer patients. He stated:
We pushed the panic button and there was a knee-jerk reaction when it was thought there would be hundreds of thousands of deaths from Covid […] However, in the event it seems we are at or near the peak and that capacity has not been needed […] We have the worst cancer survival rates compared with many of our European neighbours […] We are not in a position to cope with any increased demand at the end of lockdown.”
A leading heart surgeon, Professor Stephen Westaby, said:
…We could see thousands of deaths from heart disease and cancer over the next six months. Their families will never forget this. Neither China nor Italy stopped treating these conditions despite the chaos there earlier this year. It’s bizarre.”
How many of the additional deaths we are seeing now are caused by LOKIN-20?
Early indications from the ONS suggest the lockdown regime is having a considerable additional impact upon the nation’s health. Approximately 84% of people surveyed stated they were worried about C19. Nearly half reported an increase in anxiety levels.
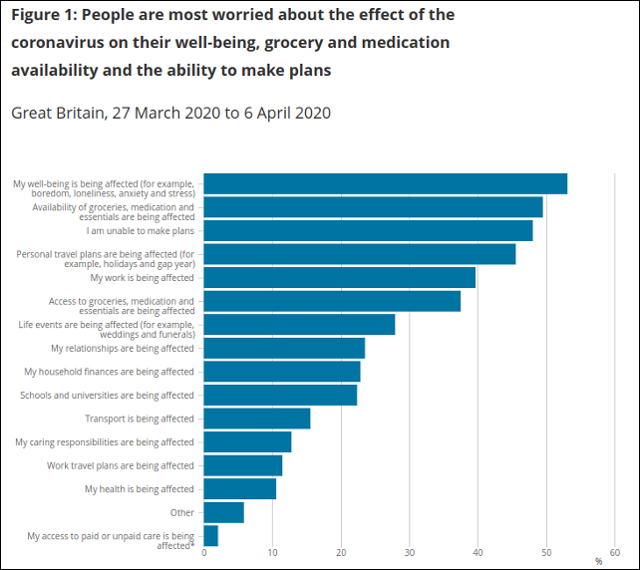
ONS Statistics on LOKIN-20 Impact Upon Mental Health In The UK
Anxiety increases the risk of cardiovascular disease and a range of other health conditions. Studies have shown a clear link between increased levels of anxiety and depression in children and adolescents. LOKIN-20 is seemingly creating a mental health crisis too.
Depression often has a lifelong impact and substance misuse, domestic abuse, low income and other comorbidities are all frequent consequences. The head of the department of psychiatry at the University of Cambridge Professor Ed Bullmore reported:
The pandemic is clearly having a major social and psychological impact on the whole population, increasing unemployment, separating families and various other changes in the way that we live that we know are generally major psychological risk factors for anxiety, depression and self-harm.”
However, it is not the pandemic that is “increasing unemployment” and “separating families” but rather the baseless lockdown regime of the State.
The kind of economic devastation caused by the lockdown regime, unlike C19, is genuinely unprecedented. The Office of Budget Responsibility (OBR) predict a 35% drop in the UK’s GDP with an additional 2 million job losses. For some reason, they envisage the UK economy will instantly recover from this hammer blow. Others are far less confident.
The Institute for Social and Economic Research (ISER) predict that nearly one quarter of UK jobs (more than 6.5 million) will be lost thanks to the lockdown. Failing to see the “bounce back” predicted by the OBR they state:
Our baseline scenario predicts an overall contraction in GDP and employment of around 20%.”

ISER predictions
Whether the OBR or the ISER predictions are accurate, it is obvious that the economic and social impacts of the lockdown regime will be catastrophic.
Social deprivations and poverty, already on the rise before the alleged C19 pandemic, are set to soar. The link between economic deprivation and mortality is not in doubt.
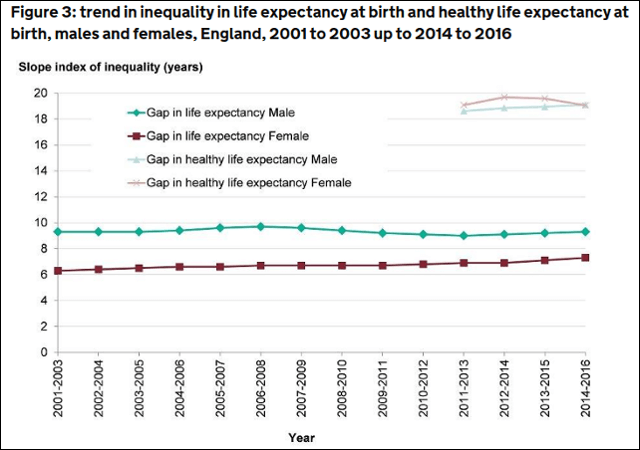
UK Government Life Expectancy Statistics
Between 2001 and 2016 economic and social deprivation in England consistently accounted for a staggering 9.3 year average reduced life expectancy for males and, by 2016, shortened women’s lives by 7.4 years. Millions of lives will be cut short by LOKIN-20.
It is a very sad reality to acknowledge that the loss of life from COVID-19 is as nothing by comparison. LOKIN-20 won’t end in a few weeks. It will continue for years to come. The longer the State persists with its destructive lockdown regime, the worse will be the consequences of LOKIN-20.
************







